


Authors: Dr. Amy de Haar-Holleman and Dr. Sofie Joris, medical oncologists at UZ Brussels (VUB)
What is pancreatic cancer?
Pancreas.
The pancreas is an organ located in the upper abdomen. It lies behind the stomach and drains into the duodenum, close to the bile ducts. The pancreas is part of the digestive system and has 2 main functions. The first is the production and secretion of juices involved in the digestion of food and the absorption of fats, sugars and proteins. The second function is the production and secretion of hormones, mainly insulin and glucagon, whose job is to control blood sugar levels.
Types of pancreatic cancer.
Pancreatic cancer occurs when cells of the pancreas derail and start dividing unlimitedly. Only 5% of pancreatic tumours arise in the cells that produce hormones. The vast majority of pancreatic cancers, 95%, arise in the cells that make digestive enzymes. Of these, the most common, over 90% is an adenocarcinoma, also known as PDAC.

Figure 1: the location of the pancreas
Symptoms in pancreatic cancer.
The symptoms that occur in pancreatic cancer can be explained by the location of the pancreas in relation to other organs. If the tumour presses on the bile ducts, the green connection between gallbladder and small intestine, jaundice will occur due to disrupted drainage of the bile. In this, the skin becomes none, the urine darkens and the skin may become itchy. If the hormone-producing cells are overgrown, diabetes or diabetes will occur. If the cells that produce digestive juices are overgrown, fatty, light bowel movements and weight loss will occur. Pressure on nerves can cause abdominal pain, which usually radiates to the back. And finally, in people with cancer in general and in those with pancreatic cancer in particular, we often see clots or clots forming in blood vessels, which can lead to a thrombosis leg, for example.
Pancreatic cancer risk factors.
There are several risk factors for the development of pancreatic cancer. In about 5-10% of people with pancreatic cancer, the cause is genetic. This means that due to the presence of an error in the hereditary material in the body cells, they have an increased risk of developing a tumour in the pancreas. We will talk more about this in the next chapter. In addition, there are other risk factors, of which smoking seems to be the strongest. The other risk factors, such as obesity, advanced age, male sex, chronic inflammation of the pancreas, alcohol, long-standing or newly diagnosed diabetes and alcohol, all also confer an increased risk of pancreatic cancer, but less strongly than smoking.

Figure 2: Risk factors for developing pancreatic cancer
How is the diagnosis made?
If you have symptoms consistent with pancreatic cancer, the GP will refer you to the hospital for further examination. During the initial consultation, a physical and a blood test will usually be done by the doctor at the hospital. In the physical examination, the doctor may see if there is a mass felt in the upper abdomen. In the blood test, the doctor can see if the organs are working properly, if there is a problem with the discharge of bile, for example, and if the tumour marker is elevated. This is a substance that some, but not all pancreatic tumours, produce and release to the blood. If there is persistent suspicion of pancreatic cancer, additional investigations will be scheduled.
There are several tests that can be done to image the pancreas. An endo-echography (EUS) is usually done. In that examination, a flexible tube with a small ultrasound machine at the end is inserted through the mouth to through the oesophagus, stomach and small intestine at the organs in the immediate vicinity, such as the pancreas, liver and gallbladder. If the tumour is seen, some tissue may be removed immediately to be viewed under the microscope, a biopsy. In addition, a CT scan of the chest and abdomen is taken to see (1) what the local situation is and whether the patient can be operated on and (2) whether there are distant metastases, for example in the liver and lungs. An MRI can be used to map the pancreas in more detail. Finally, all findings are discussed in a group of medical specialists involved in the treatment, the multidisciplinary oncology consultation (MOC). In the MOC, the treatment plan is made which is then discussed with the patient. To choose the treatment, doctors take into account the stage of the disease, the location and size of the tumour, as well as the patient’s condition, age and wishes.
Pancreatic cancer treatment
The most common treatments for pancreatic cancer are surgery (surgery) and drug treatment (chemotherapy). Sometimes radiotherapy (radiotherapy) is used, either in combination with chemotherapy or not. One of the main problems with pancreatic cancer is that symptoms do not appear until late in the course of the disease and are often diagnosed at a late stage. As a result, only in about 1 in 5 patients can the tumour be removed with surgery. Sometimes this can be done immediately, but usually the tumour must first be made slightly smaller by giving chemotherapy first. Unfortunately, in the remaining 4 out of 5 patients, the disease is only found at a late stage and there are already metastases or the tumour has not grown too much around the blood vessels. In these people, palliative treatment follows, which usually consists of chemotherapy. This treatment does not cure the disease, but it can inhibit tumour growth and thus reduce the symptoms caused by the pancreatic tumour.
Pancreatic cancer survival
At diagnosis, pancreatic cancer is classified into 4 stages. In stage I, there is a small tumour and in the pancreas and there are no metastases. Patients with stage I pancreatic cancer are the best candidates for surgery. In stage II, the tumour is larger and there may be metastases to one or more lymph nodes close to the pancreas. At stage III, in addition to the tumour, there are metastases to the lymph nodes and there may even already be progression to adjacent blood vessels. In stage IV, the pancreatic cancer has spread to organs further away from the pancreas, such as the liver, lungs or abdominal cavity. The higher the stage at diagnosis, the worse the survival. At stage I, 42% of people are still alive 5 years after diagnosis and at stage IV, only 42% are.
Genetic mutations in pancreatic cancer
Cancer results from gene defects or mutations in a cell, which usually arise by chance. Only in exceptional cases is such a defect hereditary. Gene defects occur in cells every day, but usually the cell can repair this damage itself. When the damage is too great, the cell switches itself off. In cancer, this process is different: the cell loses control, continues to divide uncontrollably and forms a tumour. This tumour can invade healthy tissues and affect other organs via metastasis.
Genetic changes that increase our risk of cancer can occur during our lifetime or be congenital (inherited). Gene mutations acquired or ‘acquired’ during our lifetime result from random errors in cell division, or from exposure to toxic substances that alter DNA such as tobacco smoke. In a minority of cases, gene mutations are congenital. In the latter case, the genetic error is passed on from parent to child. For genes that predispose to developing cancer, this occurs according to an autosomal dominant inheritance pattern which means there is a 50% chance that children will inherit the risk.
Cancer is common, making it likely that several people within one family will be affected. Although cancer can be hereditary, this is usually not the case. Hereditary predisposition plays a determining role in only 5 to 10 per cent of people with cancer.
As for the hereditary predisposition or predisposition to pancreatic cancer, several genes are known. They are divided into two major groups:
- Hereditary tumour syndromes with a >10% cumulative lifetime risk of ductal adenocarcinoma of the pancreas.
This includes patients carrying a pathogenic (disease-causing) variant in CDKN2A (hereditary melanoma), PRSS1 (hereditary pancreatitis) and STK11 (Peutz-Jeghers). - Hereditary tumour syndromes with an unknown or <10% lifetime risk of ductal adenocarcinoma of the pancreas.
This includes patients who are carriers of a pathogenic variant in BRCA1, BRCA2, ATM, PALB2, MLH1, MSH2, MSH6 and TP53.
The life-time risk of developing pancreatic cancer varies depending on the gene in which the pathogenic variant or mutation occurs and is also influenced by family history. It is important to note that this is the risk of a new cancer developing in the pancreas and is not a relapse of another cancer in the form of a metastasis (metastasis) in the pancreas.
What is the risk of pancreatic cancer for a carrier of BRCA1/2 or similar mutation?
When patients undergo genetic testing to detect hereditary breast and ovarian cancer syndrome (HBOC), the following genes: BRCA1, BRCA2, CHEK2, PALB2, ATM, MLH1, MSH6, MSH2, BARD1, BRIP1, RAD51C, RAD51D and TP53 are analysed. Only those shown in bold slightly increase the risk of developing pancreatic cancer. The risk of ever developing pancreatic cancer is 1.7% in the Belgian population. For mutation carriers, this risk is expressed as a relative risk (RR). The relative risk in this case is an estimate of the number of times the probability of developing pancreatic cancer is higher in mutation carriers compared to the general population. Of the genes belonging to HBOC, pathogenic variants in BRCA1, BRCA2 or PALB2 are the most common in families with pancreatic cancer. The syndromes with the highest risk of developing pancreatic cancer are Peutz-Jeghers syndrome and hereditary pancreatitis.
Table 1 below shows the risks for each gene.
Syndrome | Genes | Lifetime risk |
HBOC | BRCA1 BRCA2 | 2.3-3.0 RR 3.5-10 RR |
Fanconi anaemia | PALB2 | 2.4 RR |
Ataxia telangiectasia | ATM | 6.5 RR |
Peutz-Jeghers | STK11 | 11-55%, 132 RR |
FAMMM | CDKN2A | 15-20%, 47.8 RR |
Lynch syndrome | MLH1, MSH2, MSH6, (PMS2) | 8.6 RR |
Hereditary pancreatitis | PRSS1, SPINK1 | 30-70%, 69 RR |
HBOC = hereditary breast and ovarian cancer, FAMMM= familial atypical multiple mole/melanoma syndrome, RR = relative risk increase compared to general population
Early detection/prevention of pancreatic cancer
Late diagnosis in pancreatic cancer
The survival rate of pancreatic cancer is very limited for several reasons. The main reason is that the majority of cases are diagnosed late (Figure 3). As a result, surgery, i.e. cure, is no longer possible. There are several causes for the late diagnosis of pancreatic cancer.
First, pancreatic cancer typically does not produce symptoms until late in the disease process. And those symptoms, such as pain in the upper abdomen, are usually not very specific to pancreatic cancer. Second, the risk factors are not well known. Everyone knows that there is a small chance of getting lung cancer if you don’t smoke, but with pancreatic cancer it is less clear. Third, there are limitations to current diagnostics. On an MRI or endo-echography, abnormalities, especially if small, can be missed. Finally, there is no screening programme for pancreatic cancer in Belgium, as there is for breast and colon cancer, for example. Whether this is a major shortcoming is something we will come back to later in the text. All in all, the conclusion is that pancreatic cancer is usually detected at a late stage due to multiple causes and that an important way to improve survival is early detection and prevention.

Figure 3: Stage pancreatic cancer at diagnosis
Definitions: prevention, screening and surveillance
It is important to clearly understand what the different terms mean. Prevention, in this case, means lifestyle adjustments to prevent the development of the disease. For example, in the case of pancreatic cancer: not smoking, not consuming alcohol and avoiding obesity. Screening is the implementation of periodic examinations in the population for diseases that occur very frequently and by which early diagnosis is aimed. In the case of cancer, population screening exists for breast, colon and cervical cancer. Surveillance (or checks) means scheduling periodic examinations of patients known to be carriers of an inherited predisposition that increases the risk of a particular condition, in this case pancreatic cancer. If diagnosed early, before the patient has symptoms, it is often easily treatable.
Cancer prevention
The known risk factors for getting pancreatic cancer can be divided into modifiable risk factors, i.e. risk factors that you can modify yourself, and the non-modifiable risk factors, where this is not the case. Examples of non-modifiable risk factors are your genetic predisposition and your age, which cannot be changed. By removing modifiable risk factors, which can be summed up as an unhealthy lifestyle, you can slightly reduce the chances of developing pancreatic cancer. Unfortunately, it does not eliminate the risk of developing cancer.
Is screening useful?
Research has been done to determine whether a population-wide pancreatic cancer screening programme, as with breast and colon cancer, makes sense. This was found not to be the case. Because pancreatic cancer is not very common, it is a programme that would cost a lot of field, but would identify too few people. So the studies showed harm (due to overdiagnosis and overtreatment) rather than benefit for the people who underwent the screening.
Screening in people with an increased risk of developing pancreatic cancer, a high-risk population, did prove useful. A high-risk population is characterised by people having a particular genetic abnormality, i.e. error in their DNA, associated with an increased risk of developing pancreatic cancer (see Table 1). Studies in a high-risk population showed that the people who participated in a surveillance programme were more likely to have the cancer detected at an earlier stage, were therefore more likely to be eligible for surgery and had a better survival.
National and international guidelines require BRCA1/2 carriers (or carriers of another HBOC gene at risk of pancreatic cancer) to undergo periodic examinations for early detection of pancreatic cancer only if there are family antecedents of pancreatic cancer. One starts these examinations from 50 years of age or from the age at which the family member was diagnosed. Always speak to your doctor to see what is the best strategy for you.
Research into early detection/detection of pancreatic cancer
As already discussed, late diagnosis is a very important reason for the poor survival of pancreatic cancer. This makes it important to conduct research on early detection of pancreatic cancer. Fortunately, research is being conducted in several areas to further improve early detection.
Setting up a good surveillance programme actually starts with the basics. With a view to minimising the burden on programme participants on the one hand, and maximising the return on investment on the other, you prefer to offer surveillance preferably to people who are most likely to actually develop pancreatic cancer. This requires better estimation of pancreatic cancer risk, as well as better diagnostic tools.
Better estimation of pancreatic cancer risk
As mentioned, lifestyle risk factors on the development of pancreatic cancer are not strong enough to use that as a criterion for participation in a surveillance programme. By offering structured questionnaires to people with pancreatic cancer, new risk factors may be found. Most likely, the risk of developing pancreatic cancer is not determined by one, but rather the simultaneous existence of several risk factors. Once the risk factors are better mapped, an attempt can be made to create a model, from which a low, high or moderate risk of developing pancreatic cancer will emerge based on the presence and absence of risk factors.
Besides lifestyle risk factors, there are also hereditary risk factors. By looking at the DNA of large groups of patients with pancreatic cancer, a pattern of small changes in the DNA that occur in multiple patients can be found in addition to the known errors in the genetic material. As with lifestyle risk factors, the hereditary risk factors can also be incorporated into a model, from which a low, high or moderate risk of developing pancreatic cancer emerges based on presence and absence of risk factors. Such a model is called a polygenic risk score.
A risk score based on the presence and absence of lifestyle and genetic factors is expected to give the best prediction. However, making these risk models as accurate as possible requires a very large effort with data from thousands of patients.
Better pancreatic cancer diagnostics: biomarkers
A biomarker is a measurable substance in the body that says something about the presence of a disease. In our context about the presence of pancreatic cancer. Biomarkers can be measured in all body fluids, but in practice are often measured in the blood. Currently, when a blood sample is taken from someone with suspected pancreatic cancer, the tumour marker Ca19.9, among others, is determined. An ideal tumour marker is made only by the tumour and not, or hardly, by normal body cells. Ca19.9 is not an ideal tumour marker because, firstly, it is not produced by all pancreatic cancers and, secondly, it is also produced in response to other causes, such as problems with the bile ducts.
Ca19.9 is an example of a protein that a pancreatic tumour can produce. The search for a good tumour marker goes beyond the protein level. Other traces of a tumour can also be found in body fluids such as blood, urine and saliva. Circulating tumour cells that have detached from the tumour or even the tumour’s hereditary material (DNA, RNA or microRNA) can also be found in the blood. Also metabolic products of the tumour (metabolites). These products can be found loose in body fluids, but are also sometimes found in fatty vesicles (exosomes). Also, immune cells may make a defence reaction against the tumour, resulting in tumour-specific antibodies.
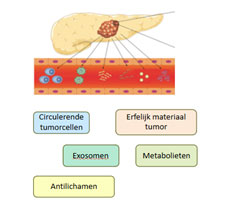
Figure 4: Examples of diagnostic biomarkers in pancreatic cancer
International cooperation
To arrive at new diagnostic biomarkers and risk factors in a disease as relatively rare as pancreatic cancer, it is necessary to join forces internationally. Several initiatives have been established with this aim.
PRECEDE is a consortium in which hospitals in both the United States and Europe participate. Within PRECEDE, people at high risk of developing pancreatic cancer are offered a surveillance programme. Participating hospitals take questionnaires and blood, urine and saliva samples from patients participating in the programme and send them to a central point in America. Here, the samples are stored and later analysed. The answers to the questionnaires are fed into a large research database. Powerful computers work with this to try to create risk models using this data. The UZ Brussel is in the process of becoming part of PRECEDE, but due to different legislation in America and Europe, this is a challenging process. The CAPS consortium is an example of a similar, somewhat smaller, initiative.
